If you have been told you have fibroids and you are trying to conceive, it is normal for your mind to go straight to one question: can fibroids cause infertility? The honest answer is that they can, but not always. Many women get pregnant with fibroids and have healthy pregnancies. Others find that fibroids get in the way, especially depending on where they sit in the uterus and how large they are.
The tricky part is that fibroids are common, symptoms can be confusing, and fertility problems often have more than one cause. This guide breaks it down so you can understand what's important, what questions to ask your doctor, and what treatments are usually suggested.
What Are Fibroids?
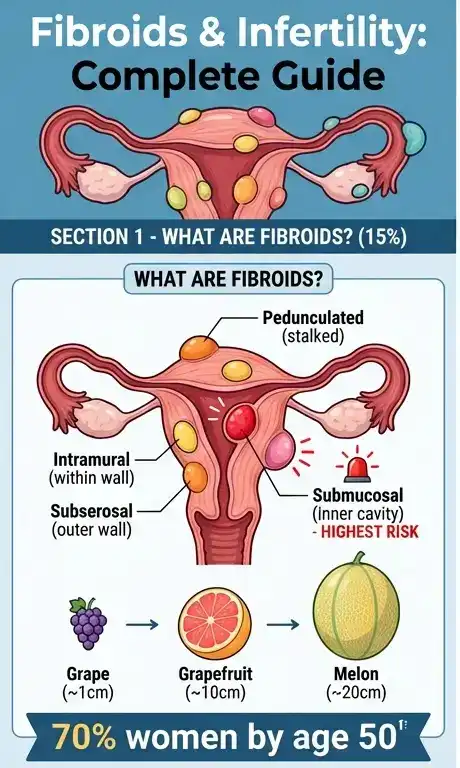
Fibroids, which are also called uterine fibroids or leiomyomas, are muscle and connective tissue growths that form in or on the uterus.
A few reassuring facts upfront:
- They are very common, especially in women in their 30s and 40s.
- They are usually non-cancerous.
- Many women have fibroids and do not even know it.
Fibroids can be tiny like a seed or large enough to change the shape of the uterus. When it comes to fibroids and fertility, the part of the uterus where they grow is also very important.
Doctors often describe fibroids by location:
- Submucosal: grows into the uterine cavity (the inside space where pregnancy implants)
- Intramural: grows within the uterine wall
- Subserosal: grows on the outer surface of the uterus
- Pedunculated: attached by a stalk (inside or outside)
Can Fibroids Cause Infertility?
Yes, uterine fibroids infertility can happen, but it depends. Fibroids do not automatically mean you will struggle to get pregnant.
Here is the balanced reality:
- Some fibroids don't affect fertility at all, especially small fibroids on the outside of the uterus.
- Other fibroids can make it harder to get pregnant by changing the shape of the uterus, making it harder for the embryo to implant, or getting in the way of sperm movement.
Three things tend to matter most:
- Location: Fibroids that distort the uterine cavity (especially submucosal fibroids) are the most linked with infertility and miscarriage risk.
- Size: Bigger fibroids are more likely to cause problems, but even small ones can be a problem if they are in the "wrong" spot.
- Number: Having more than one fibroid can sometimes have a bigger effect on how the uterus works than having just one.
Also, infertility is often caused by more than one thing. If someone has fibroids and trouble conceiving, the fibroids might be the main issue, or they might be one piece of a bigger picture (ovulation, sperm quality, tubal issues, age-related egg quality, endometriosis, thyroid problems).
So the best next step is not to panic. It is a good evaluation.
How Fibroids Affect Fertility
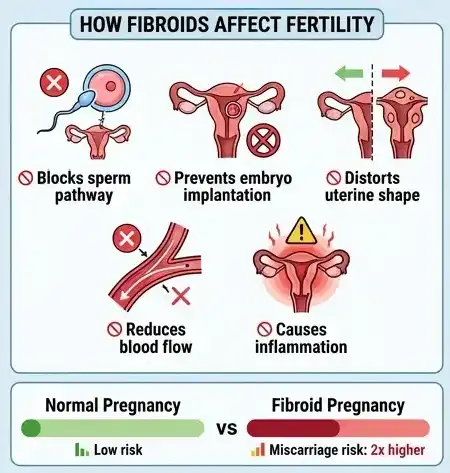
When fibroids do cause fertility problems, it is usually through a few key mechanisms. You might not feel any symptoms and still be affected, which is part of why this topic gets frustrating.
Implantation issues
A pregnancy needs a healthy place to implant. If a fibroid bulges into the uterine cavity, it can:
- reduce available space for implantation
- disrupt the uterine lining
- increase inflammation in the area
Submucosal fibroids are the most likely to interfere here.
Changes in uterus shape
Fibroids can change the shape of the uterus, especially if they are large or multiple. That can affect:
- how sperm travels through the uterus
- how an embryo moves and implants
- how the uterus contracts (uterine “peristalsis”)
Blood flow interference
Some fibroids may alter blood flow to the uterine lining. Adequate blood supply is important for implantation and early pregnancy development. The exact relationship is still being studied, but many fertility specialists take fibroid size and location seriously for this reason.
Cervix or fallopian tube effects (less common, but possible)
A fibroid near the cervix or close to the fallopian tube openings may make it harder for sperm to reach the egg. This is not the most common scenario, but it does happen.
Common Symptoms of Fibroids
Some women feel nothing at all. Others have symptoms that slowly become “normal” over time because they have lived with them for years.
Here are practical symptoms of fibroids to watch for:
- Heavy periods (soaking through pads or tampons quickly)
- Periods that last longer than usual
- Passing clots during menstruation
- Pelvic pressure or a “full” feeling in the lower belly
- Frequent urination (from pressure on the bladder)
- Constipation (if a fibroid presses on the bowel)
- Pain during sex (not always, but it can happen)
- Lower back pain
- Bloating that does not match your diet changes
- Trouble getting pregnant or recurrent early pregnancy loss (in some cases)
If you have heavy bleeding, it is also worth checking iron levels. Low iron can sneak up on you and cause fatigue, shortness of breath, and dizziness.
Can You Get Pregnant with Fibroids?
Yes, many women ask can you get pregnant with fibroids, and the answer is often “yes.”
A lot depends on the fibroid type:
- Small subserosal fibroids (outside the uterus) often do not affect fertility much.
- Intramural fibroids can be a gray area. Some seem harmless, while others may lower fertility if they are large or distort the cavity.
- Submucosal fibroids are the most likely to interfere with conception and implantation.
Even if you do get pregnant, fibroids can sometimes cause issues during pregnancy, like pain from fibroid degeneration, higher risk of bleeding, or changes in placenta placement. Many women still carry to term without major problems, but it is something your OB-GYN will monitor.
If you are trying to conceive and you know you have fibroids, ask your doctor about imaging that shows cavity involvement, such as:
- transvaginal ultrasound
- saline infusion sonogram (SIS)
- hysteroscopy (in some cases)
- MRI (sometimes used for complex cases)
These tests help answer the question that really matters: is a fibroid affecting the space where pregnancy needs to grow?
Treatment Options for Fibroids
Fibroids treatment is not one-size-fits-all. The “right” plan depends on your symptoms, your age, your fertility goals, and the fibroids themselves.
If pregnancy is your goal, treatment decisions often focus on two things:
- improving the chance of conception
- reducing miscarriage risk
Medical Treatment Options
Medications do not always shrink fibroids permanently, and they usually do not “remove” them. Still, medical treatment can play a helpful role, especially when symptoms like heavy bleeding need control or when hormonal support is needed during fertility treatment.
In some cases, doctors may suggest medications that help regulate hormones or support ovulation, particularly if fibroids are not the only issue.
Hormonal treatments (general examples):
- Birth control pills or hormonal IUDs to manage heavy bleeding (not used when actively trying to conceive)
- GnRH agonists or antagonists to temporarily shrink fibroids before surgery (used in selected cases under specialist care)
Fertility support medications (when appropriate):
If ovulation is irregular or luteal support is needed, your doctor might recommend:
- Progesterone support such as Susten or Duphaston (often used to support the uterine lining in certain fertility plans). You can see examples under hormonal treatment options and fertility support medications.
- Ovulation support medications from the clomiphene group, like Clofert or Siphene, sometimes used when ovulation is a concern. See ovulation support treatments.
- HCG trigger injections such as Ovidac or Hucog, commonly used in timed intercourse or assisted reproduction cycles. See fertility support medications.
These medications are not “fibroid cures.” They are more about supporting the cycle, ovulation, or early pregnancy conditions when a clinician believes it is helpful.
It’s always better to speak with a doctor before starting any treatment.
Hormonal Balance Treatment
Fibroids are thought to be influenced by hormones, especially estrogen and progesterone. That does not mean hormones are the only cause, but they are part of the story.
In some fertility situations, clinicians may address hormonal balance or uterine lining preparation. This is where medications like Progynova or Premarin may come up in care plans for some patients. These are prescription hormonal therapies and should only be used under medical supervision.
If you are seeing these names online, it does not mean you need them. It just means there are tools doctors sometimes use depending on the diagnosis.
Surgical Options (Brief, balanced)
When fibroids are clearly interfering with fertility, surgery is often discussed, especially for submucosal fibroids.
Common procedures include:
- Hysteroscopic myomectomy: uses a scope to remove fibroids from inside the uterus without making any cuts in the abdomen. Commonly evaluated for submucosal fibroids.
- Laparoscopic or open myomectomy removes fibroids from the wall or outer surface of the uterus. This can help in some situations, especially when there are a lot of fibroids or they are big.
- Uterine artery embolization (UAE): cuts off the blood supply to fibroids, which makes them smaller. It is not usually the first choice for women who want to get pregnant because it can sometimes affect the function of the uterus or ovaries.
- Hysterectomy: removes the uterus and ends fertility. This is usually reserved for severe symptoms when pregnancy is not desired.
Surgery always comes with trade-offs, like scarring or recovery time. Still, for certain fibroid types, especially those distorting the cavity, surgery can significantly improve pregnancy outcomes. Your doctor can help weigh the risks based on your specific imaging.
Lifestyle and Natural Support
Lifestyle steps will not “melt away” fibroids overnight. If you see claims like that, be skeptical.
Still, healthy habits can support your body and may help with symptoms:
- Maintain a healthy weight: body fat affects estrogen levels, and weight can influence symptoms.
- Manage iron intake: if bleeding is heavy, iron-rich foods (and supplements if advised) can help prevent anemia.
- Prioritize sleep and stress reduction: stress does not “cause” fibroids in a clear proven way, but chronic stress can worsen your overall hormonal balance and cycle regularity.
- Limit alcohol and avoid smoking: both are linked to worse overall reproductive health.
- Vitamin D: some research suggests low vitamin D is associated with fibroids, but it is not fully settled. Checking levels with your doctor is a reasonable step.
Think of lifestyle support as strengthening the foundation, not replacing medical care when fibroids are clearly a problem.
When Should You See a Doctor?
If you are trying to get pregnant and have fibroids, seeing a doctor early can save months of guesswork.
Make an appointment if:
- You have been trying to conceive for 12 months (or 6 months if you are over 35)
- Periods are very heavy, long, or painful
- You have pelvic pressure or pain that affects daily life
- You have had miscarriages or repeated implantation failure
- Your doctor has already seen fibroids on imaging and you want a fertility-focused plan
A fertility specialist or OB-GYN can help determine whether the fibroids are likely “bystanders” or part of the cause.
FAQs
Can fibroids cause infertility?
Yes, fibroids can cause infertility in some women, especially when they are inside the uterine cavity or distort it. Location matters more than almost anything. Many women with fibroids still conceive naturally, so a proper evaluation helps you understand whether your fibroids are likely affecting your fertility or not.
Can I get pregnant with fibroids?
In many cases, yes. You can get pregnant with fibroids, particularly if they are small and not affecting the uterine cavity. Some fibroids can increase the risk of miscarriage or complications, so it is smart to get imaging and a plan with your OB-GYN, especially if you have had trouble conceiving.
Do fibroids need treatment?
Not always. If fibroids aren't causing any problems and aren't making it harder to get pregnant, doctors may suggest "watchful waiting." If fibroids cause heavy bleeding, pain, anemia, or problems getting pregnant, treatment is more likely. The best approach depends on your symptoms and whether you are trying to get pregnant now.
What size fibroid is dangerous?
There is no single “dangerous” size. A smaller fibroid in the wrong place can affect fertility more than a larger fibroid on the outside of the uterus. Doctors look at size, location, how fast it is growing, and symptoms like heavy bleeding. If a fibroid causes severe pain, heavy bleeding, or rapid growth, get evaluated promptly.
Can fibroids go away on their own?
Fibroids sometimes shrink after menopause when estrogen levels drop. Before menopause, fibroids may stay the same size, grow slowly, or occasionally shrink a bit. It varies. There is no reliable natural method proven to eliminate fibroids completely. If symptoms are significant or fertility is affected, medical guidance is important.
Does removing fibroids improve fertility?
It can, particularly when fibroids alter the uterine cavity. Studies generally show that removing submucosal fibroids increases the chances of getting pregnant. The advantage for intramural fibroids is contingent upon their dimensions and their impact on the cavity. Your doctor will use imaging results to guide whether surgery is likely to help.
Final Thoughts
So, can fibroids cause infertility? Sometimes, yes. But it is not a guaranteed outcome, and it is not a reason to lose hope. Fibroids are common, and many women with fibroids conceive naturally. When fibroids do interfere, it is usually related to where they are located and whether they change the inside shape of the uterus.
If you are worried about fibroids and fertility, the most helpful step is a clear diagnosis with imaging and a plan that matches your goals. Treatments range from monitoring to medication support to surgery, and a good doctor will talk you through the pros and cons without rushing you.
It’s always better to speak with a doctor before starting any treatment.